


Remission Returns With Daily Ivermectin. No Gel/plastic, Rubber Clot in Blood.
In the prior post I demonstrated gel/plastic (g/p), rubber clot, in my blood when I was taking oral ivermectin and oral chlorine dioxide every other day. I wanted to achieve remission.

In prior posts I showed adding ivermectin (ivm) suppressed g/p, rubber clot, in my blood when tested using a plain 10 ml vacutainer tube and centrifuge. I recently decreased the oral ivm to every other day and saw g/p, rubber clot, return. I wanted to definitively show that chlorine dioxide was not necessary to achieve remission.
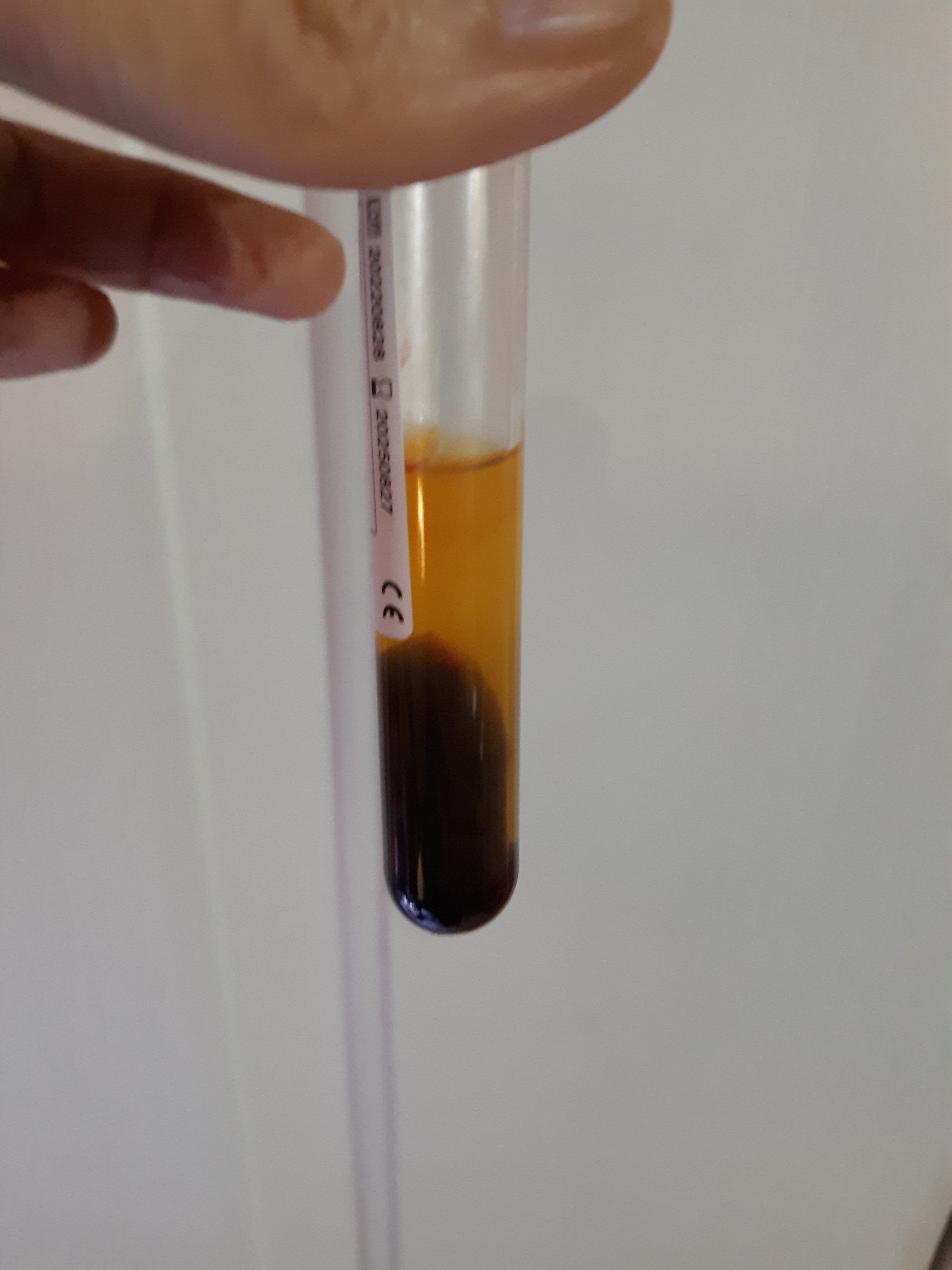
In this test I increased the ivm from every other day to a daily dose of 10 mg (1 ml) orally. I did a plain 10 ml vacutainer test on day 3 of this treatment and g/p, rubber clot, remained. A repeat plain vacutainer test on day 5 of the daily ivm showed remission and no g/p, rubber clot, was detectable. The following picture shows the plain vacutainer tube with my blood which has capacity to show g/p, rubber clot, when taken outside of this treatment. Note that the serum above the packed red cells is clear and shows no evidence of g/p, rubber clot.
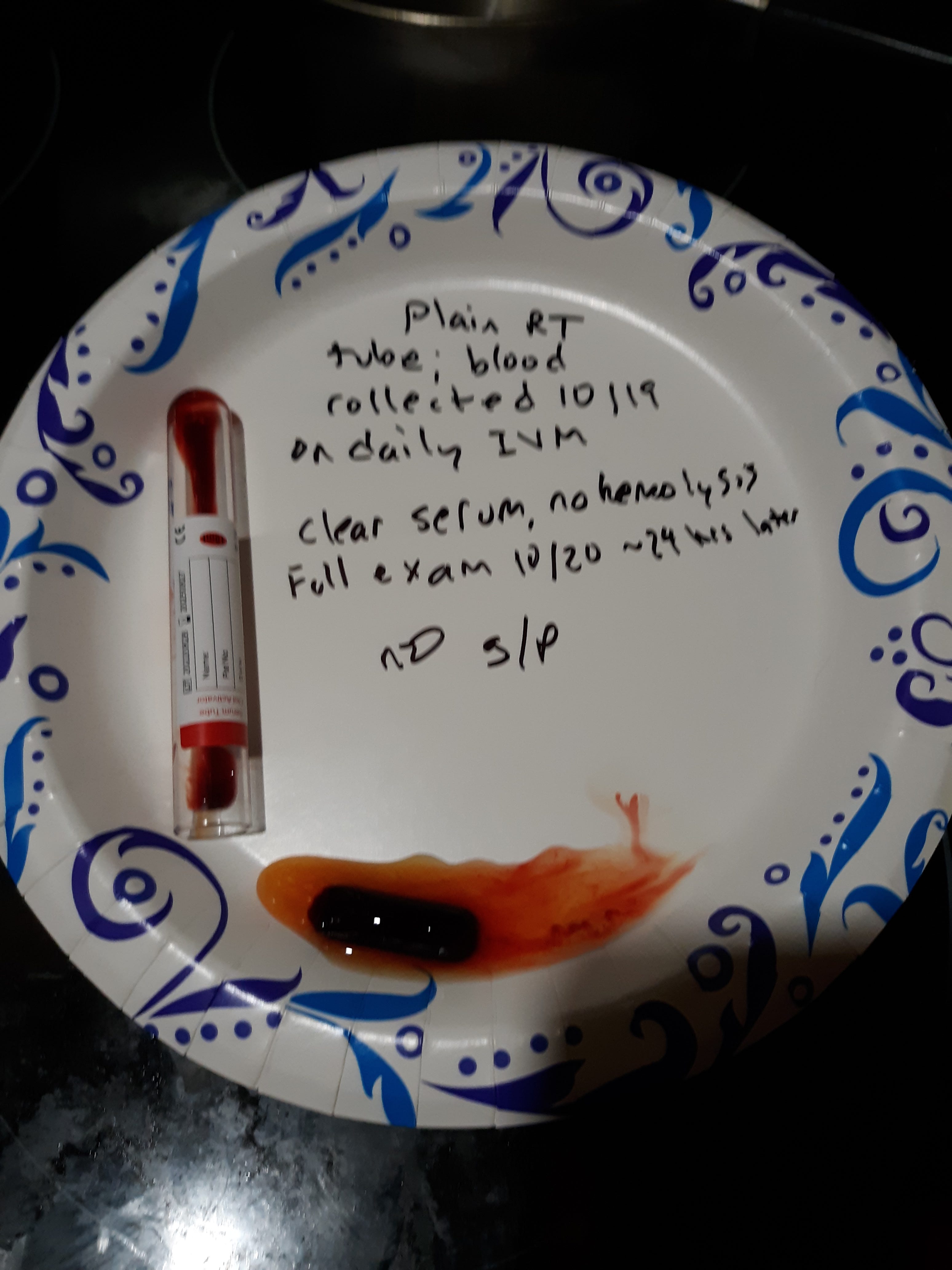
The following picture shows the vacutainer tube contents fully examined about 24 hours after the venipuncture collection and centrifuge process. No g/p, rubber clot, is present.
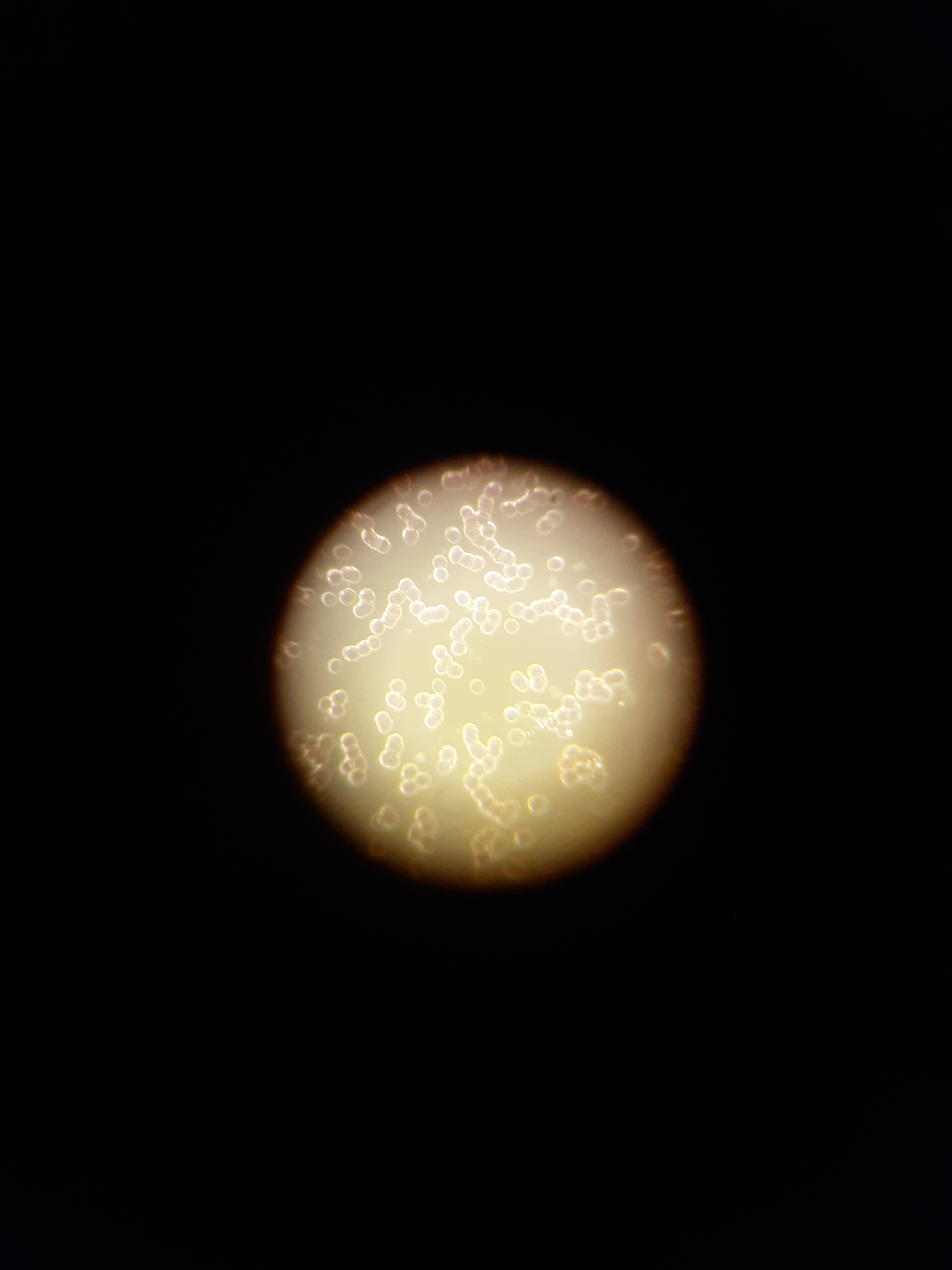
The following picture is from life blood analysis taken in the present state of no g/p, rubber clot, by vacutainer tube testing. Minimal rouleaux is seen and red cells appear with well formed margins.
Summary and discussion. I have demonstrated on several occasions that holding ivm treatment allows the return of g/p, rubber clot, in my blood. I have shown adding ivm orally to my treatment regimen caused g/p, rubber clot, to be suppressed on several occasions. It seems in my case that adding the low dose ivm orally, takes about five days to suppress g/p, rubber clot formation in my blood. It appears chlorine dioxide is not necessary to achieve this suppression. The only reason I am testing chlorine dioxide is that it was also taken along with ivm when by serendipity, I was trying to avert a sinus infection, I discovered my g/p was suppressed. So this recent testing confirms chlorine dioxide is not needed to suppress g/p, rubber clot. It does not mean it is not useful but not required here. I am unsure if ivm alone is required to achieve suppression of g/p, rubber clot, since I am taking 4 fibrin proteases, along with oral EDTA and topical EDTA (and other nutraceuticals listed in prior post). I will say I was taking the proteases and EDTA for many months and they did not prevent g/p, rubber clot, formation. My weight is 140 lbs and the daily oral dose I took was about 10 mg (1 ml of the liquid form that uses 1 ml per 100 lbs cattle weight). I do not recommend any med to any individual. Check with your health care professional before starting any new treatment. This dose is below the initial dose of 0.2 mg / kg that was used in the initial pandemic but was increased to 0.6 mg / kg during delta strain. Although ivm is listed on the WHO's list of essential meds, I don't know of studies looking at ivm used daily for long term. It does appear spike may be produced in some individuals indefinitely and may require long term meds for suppression.
As in prior posts I recommend that you consider taking the proteases after consulting your health care provider (lumbrokinase, serrapeptase, nattokinase, and bromelain) in that I have shown they can dissolve preformed cubes of g/p when placed in a solution containing any one of these as well as stop the expression of g/p when added to a tube of my blood. The proteases also have shown by many other studies to have a cardiovascular benefit and/or wound healing benefit. Many truth doctors like Dr Peter Mccullough and Dr Pierre Kory advocate their use.
The same cardiovascular benefits are attributed to EDTA use, and that are maybe related to its ability to chelate heavy metals. Dr Ana Mihalcea is an EDTA advocate.
This is just conjecture on my part but maybe the g/p, rubber clot, is a scaffold for the nanotechnology to be distributed throughout the body and a suppression at the g/p, rubber clot level can curtail some of the damage.
The late German pathologist, Arne Burkhardt, gave a presentation about g/p, rubber clot, and that it contained spike, fibrin, and amyloid. Amyloid proteins maybe found as a result of a tissue not being able to breakdown a component found there. In prior posts I gave a link that showed spike proteins when acted on by neutrophil elastase can form amyloid fibrils and that fibrin when stretched and recoiled can form beta pleated sheets. This secondary structure of proteins is common in amyloid and appears to be a component in g/p. Dr Burkhardt ‘s presentation can be seen on Rumble. Use his name to search and it’s from 7 mths ago and 38 min in duration. For some reason the link will not post here.
If Dr Burkhardt is correct then spike causes a tremendous inflammatory process in many if not all tissues in the body. It appears that shedding does occur and everyone is at risk and continuous production of spike can occur. Let’s look at some of the mechanisms that ivm has against spike. Please see this link for details: The J of Antibiotics, The Mechanisms of action of Ivermectin against SARS-CoV 2; 75, 60- 71, 2022. Ivm inhibits binding of spike to Ace 2 and CD 147 receptors. It inhibits RdRp ( RNA dependent RNA polymerase which is needed to duplicate the genetic materal) and inhibits a viral protease that is needed to cut up the initial polyprotein generated. Ivm inhibits the cytokine storm by inhibiting MAP 3 kinases and NF kb pathway. It inhibits several pathways that result in pulmonary fibrosis and resulting poor lung function. It inhibits t-PA that would increase thrombus (blood clot) formation. Dr Burkhardt makes a connection with the spike and inflammatory pathways it is involved in to SAD (sudden adult death). Tom Haviland sent out 179 questionnaires to embalmers in North America and overseas and 50 % of the embalmers are seeing the rubber clots. Richard Hirshman an embalmer in the US states that about half the bodies he sees have the rubber clots.
Again I state we need more individuals testing for evidence of g/p, rubber clot, by plain vacutainer tube test and use of a centrifuge. See prior posts on how to test and we need others to test theraputics.
The fool has said in his heart. “There is no God.” They are corrupt. They have done abominable works, There is none who does good. Psm 14 :1
My centrifuge has arrived! I showed g/-p a month ago. I have been taking artemisia and nattokinase for 3 weeks. I will check a sample shortly and let you know. Thanks for your leadership Ron!
Hi Ron,
I am taking only ivm and am on day 2. Haven't had any other protocol for a week prior. I would consider my g/p and fibre count to be average compared to the may i see every day now.
Spun my blood the day prior to starting (its still the same) and have measured the G/P. Will do so again on finishing 5 days of ivm. It will at least give a comparison.
I agree fully with your assessment that removing the g/p may be a key factor and hope that's correct.
Again, Thank you for your diligent work and setting a standard for us all.
(deleted comment was a copy of the same comment that appeared upon posting)