


If You Halt the Tissue Destruction of Spike, Can You Decrease the Incidence of Sudden Adult Death Syndrome (SADS)?
In the past post I had planned to increase the oral dosage of ivermectin and stop any protease contribution to the destruction of gel/plastic (g/p), rubber clot. Let's see the results.

In the past when I held the four proteases (lumbrokinase, serrapeptase, nattokinase, and bromelain) for three days but still taking low dose ivm orally daily (1ml = 10 mg), I had return of g/p, rubber clot. I felt I could overcome the protease contribution by increasing the ivm ( I had seen adding ivm to my treatment in the past brought remission and heard of others taking ivm recently and achieving remission). I increased the daily oral ivm to 2 ml (10 mg/ml of type that recommends 1ml/ 100 lbs cattle weight). My weight is 140 lbs (64 kg) so I was taking about 0.3 mg/kg. Remember during the pandemic ivm dosing was initially 0.2 mg/kg but increased to 0.6 mg/kg during delta strain.
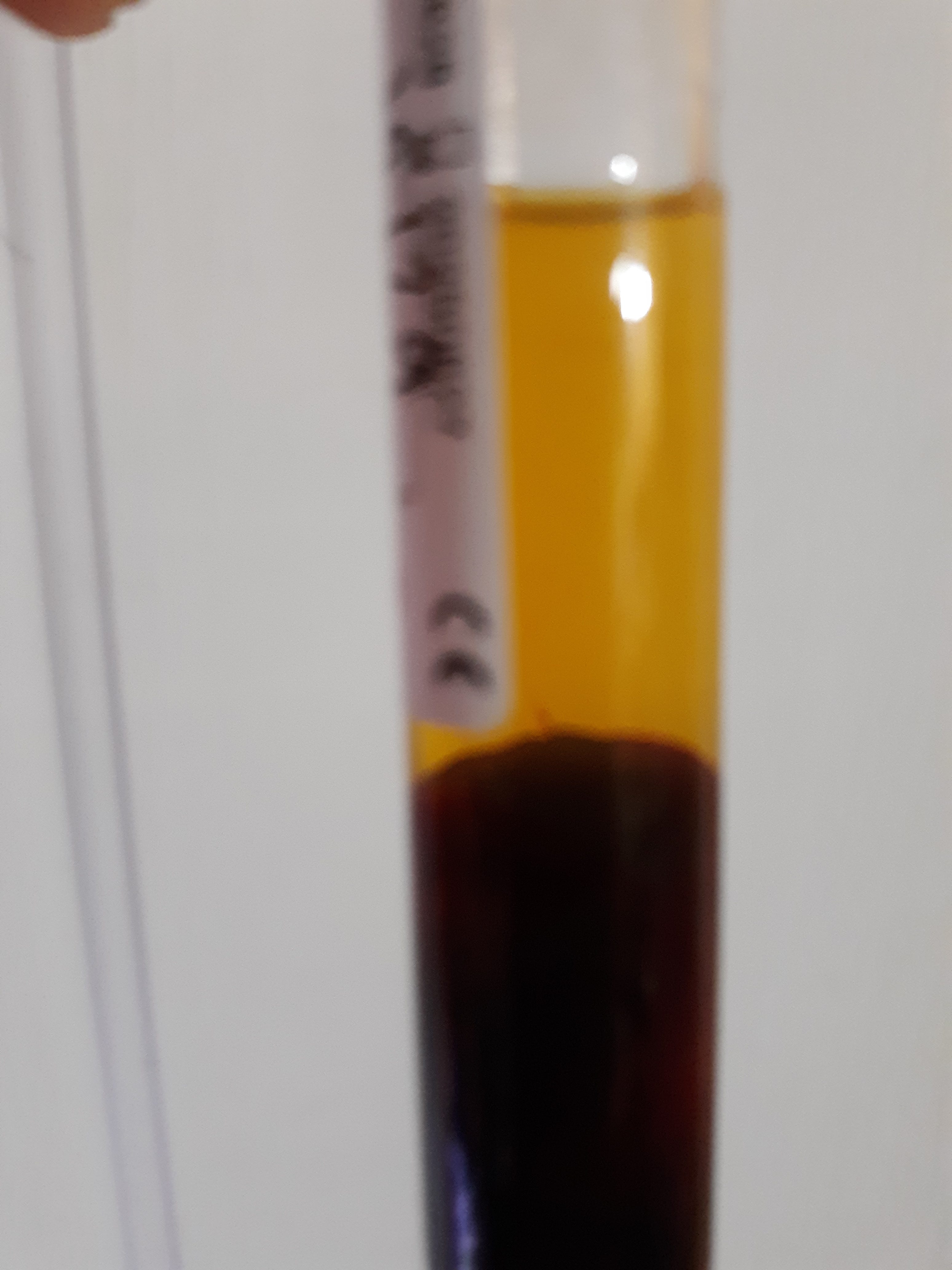
Let's look at the results. The following picture is of the plain vacutainer tube which contains my blood that in circumstances not undergoing treatments contains g/p, rubber clot. The blood was collected by venipuncure into a 10 ml plain red top tube, mixed gently by inverting tube x10, waiting 30 min, and then centrifuged at 3k rpm for 30 min. Visual inspection of the tube shows a slanted whisp of light cloudiness above the packed cells that maybe be suspicious for g/p, rubber clot.
The following picture shows complete examination of the tube contents after refrigeration overnight and approximately 24 hrs after blood collection. The serum is clear and the whisp of gray is consistent with g/p after rinsing and drying. The final volume of g/p after rinsing in tap water was 0.012 ml. This is the smallest amount of g/p, rubber clot, that I have ever detected in myself.
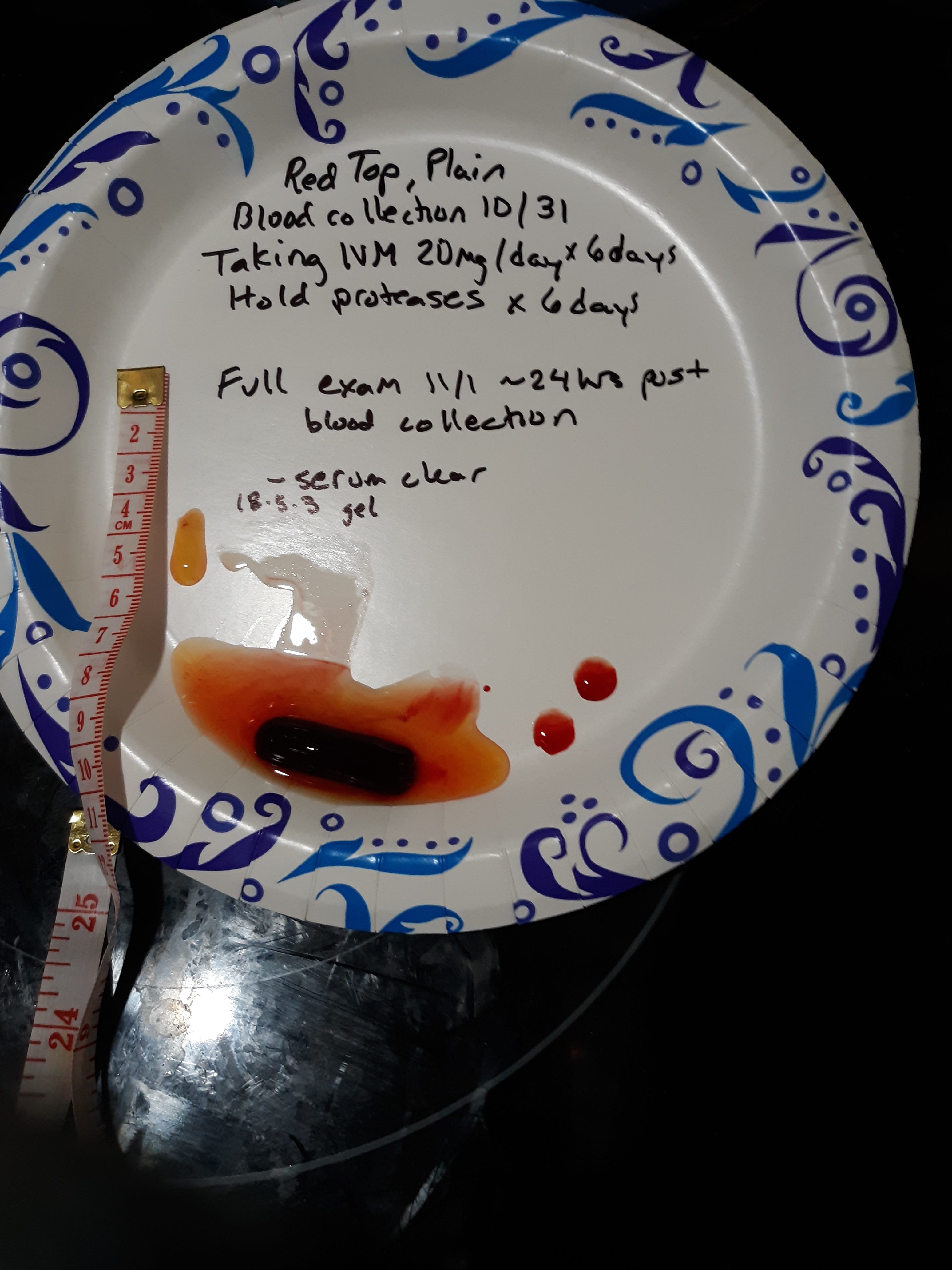
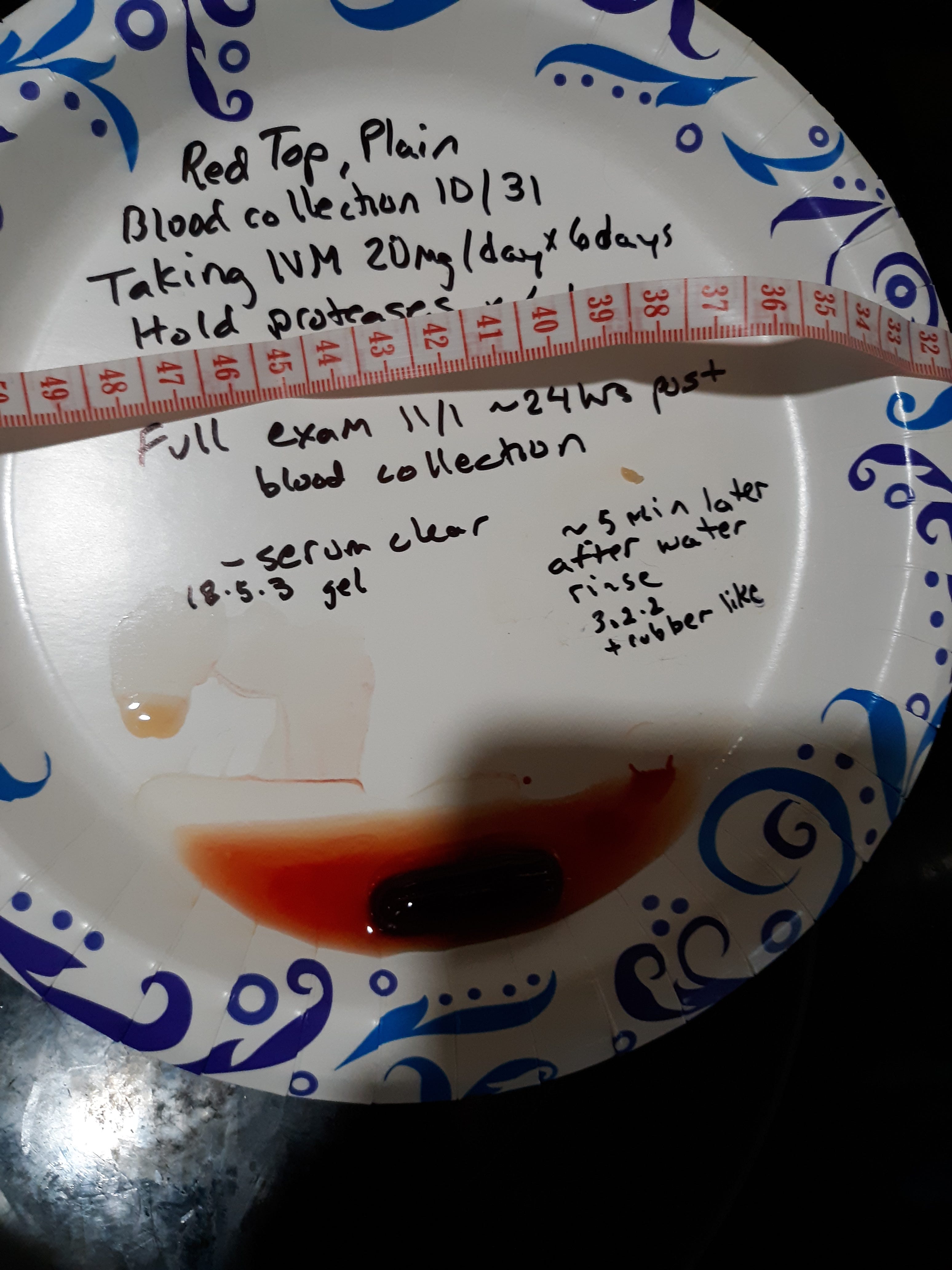
This finding is when I was taking 2 ml ivm orally/day x 6 days and holding any of the four proteases as well as holding the oral and topical EDTA. I did not show the results but I also did the test on day 4 of holding the proteases and EDTA and found g/p rubber clot with a volume of 0.03 ml (while still taking 2 ml ivm). So I was unable to suppress g/p, rubber clot, with ivm alone (discounting minor nutraceuticals) at a dose of 0.3mg/kg daily for 6 days.
Summary and discussion:
Let me again present the findings of the late German pathologist, Arne Burkhardt, showing an intense inflammatory response in the vessel endothelium (inner most lining of blood vessels) which leads to destruction of the vessel walls he called endotheliitis and when it involved the middle layer he called media necrosis. This destruction of vascular tissues was washed down stream along with uncontrolled production of spike forming the g/p, rubber clot. Here is a link to a video from January of this year.
https://rumble.com/v2bnvdm-pathologist-dr.-arne-burkhardt-autopsies-show-the-mrna-vaccine-shreds-peopl.html
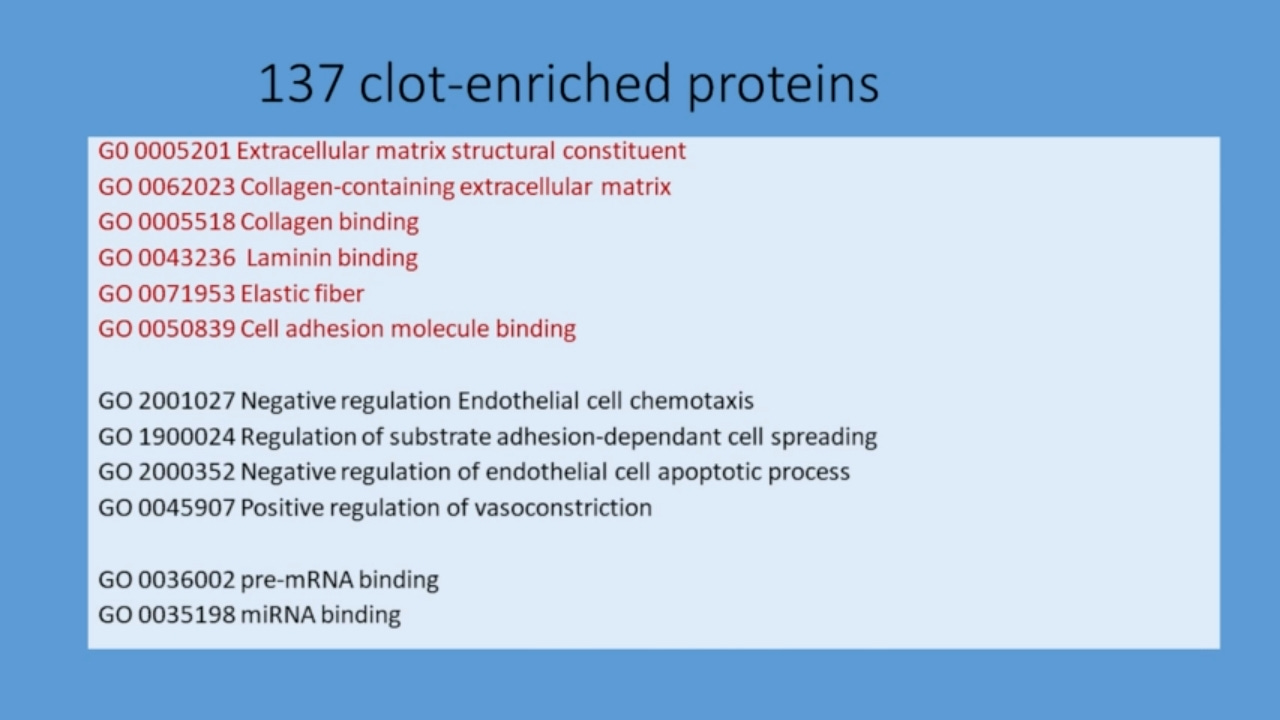
The following is a slide from Dr Burkhardt's presentation showing 137 proteins that were identified in the g/p, rubber clot, compared to the serum in the same tube and six were specific to endothelium.
Dr Burkhardt as well as Dr Ryan Cole have shown slides that show g/p, rubber clot, stains positive for spike and I will add a link that shows spike when acted on by neutrophil elastase (a protease) can form amyloid fibrils (J Am Chem S 2022, 144, 20, 8945-8950). In normal blood coagulation several serine proteases are produced and maybe act like neutrophil elastase and cut the intact spike to form amyloid fibrils. This would also explain why blood needs to coagulate to get g/p, rubber clot. Fibrin is also present in the g/p, rubber clot, and is also able to form beta sheet configuration that can bind Congo red stain allowing identification as amyloid. Here us a reference to a paper that connects spike to amyloid to hydrogel.
We also have destruction of vessels and various proteins in a soup mix washing down the blood stream. So to summarize the spike causes an inflammatory destruction of the vessel walls that wash down with spike and g/p, rubber clot components (a hydrogel). This destruction of the vessel wall leads to aneurysms and clots with obstruction that can cause SADS. The following slide is from Dr Burkhardt ‘s presentation.
It seems probable that stopping the vessel destruction could decrease the incidence of SADS. In my last post I proposed that two classes of med for this problem of g/p, rubber clot, exists. One class would include ivm that prevent the destruction of the vessel wall and its consequences. Some of the mechanisms of ivm can be found at J of Antibiotics, The Mechanisms of Action of Ivermectin Against SARS CoV 2, 75, 60 -71, 3022. Remember it can inhibit binding of spike to ACE 2 receptor on the endothelium and inhibit multiple pathways leading to a cytokine storm (inhibition of MAP 3 kinases, NF kb, STAT 3, PAK 1 and more!)
The other class of meds deals with the disposal of the breakdown products of the vessel wall and it is unclear to me if this class changes the disease course if vessel wall destruction has occurred. Fibrin proteases are in this latter class since they help dissolve the g/p, rubber clot after the fact of vessel wall destruction. But another benefit of the proteases is that in a paper by Tanikawa (Degradative Effect of Nattokinase on Spike Protein of SARS CoV 2, Molecules 2022) natto can breakdown spike on cell surface and contribute to a beneficial effect prior to any vessel wall destruction. Another paper by Oba, (Biochem Biophys Res Commun. 2022 Sep 17; 520: 21-25) he found the SARS CoV 2 receptor binding domain was proteolytically degraded so this would be a benefit prior to any vessel wall destruction.
I suspect chelators are in the class of meds that prevent hydrogel (rubber clot) formation after vessel wall destruction has occurred. In a prior post I took vacutainer tubes containing either EDTA or citrate which binds the calcium needed as a cofactor for clotting and after centrifuge, no g/p, rubber clot was detectable. If I added calcium to the same tube and gently agitated the tube, waited 30 min, centrifuged, then the normal clotting process occurred, and I got g/p in the tube. So in the presence of EDTA the rubber clot could not be expressed but one could argue the pre components of the rubber clot remained and if they are composed of destroyed vessel wall components, then EDTA works after the destruction has occurred. What happens in a test tube maybe far different than in the body's open system. In the experiment shown above I held EDTA (oral and topical) for 4 days as well as holding proteases. It was not wise of me to also stop the EDTA (oral and topical) at the same time as I stopped the proteases since I can't say the absence of which one allowed g/p to remain. Let me say I cannot rule out some beneficial effect of metal chelators prior to vessel wall destruction either, but I can't think of a mechanism.
Anyway if you stop the vessel wall destruction (and stop spike) or you dispose of the breakdown products, the confirmatory test (like vacutainer tube with centrifuge use) would look the same and no g/p, rubber clot, would be present but the way you got the negative result may make a huge difference in prognosis.
I think one of the first steps is to see if you have g/p, rubber clot in your system. I have found it in the vaccinated and unvaccinated. I have also not seen it in vaccinated and unvaccinated. Spike seems to be expressed long term in some individuals and Dr Burkhardt stated that some have an ongoing endotheliitis. You need to know for sure if you have it prior to considering taking something daily forever? As I have always stated I am sharing my experience and my findings. Check with you health care provider for your particular case.
I personally would take at least a single protease (lumbrokinase, serrapeptase, nattokinase, bromelain) as well as EDTA since each of these have literature reports of cardiovascular benefits (some have arthritis or wound healing benefits). Since I have shown that the proteases can add to a suppression of g/p, rubber clot, I will test if nattokinase along with ivm can restore remission from g/p, rubber clot. I have already shown ivm and the 4 proteases plus the oral and topical EDTA can suppress g/p, rubber clot. I have not shown ivm alone can suppress g/p. I will need to try a higher dose than 0.3 mg/kg daily in the future (and without the proteases and EDTA).
As I stated before, I don't know the origin of spike ( CDB, LNP, EMF, etc) or even what it is and these findings do not negate aggravating factors known or unknown in this disease. Is there further contribution to the soup of g/p, rubber clot, other than breakdown products of vessel destruction and the foreign spike? For instance some other hydrogel also being produced along side the tissue destruction? This did not show up in the analysis by Dr Burkhardt. Is there some other yet unidentified metal (could be calcium) that when chelated keeps the hydrogel from forming? And if that metal undergoes a redox change it loses its ability to allow hydrogel to be expressed? That could explain why hemolysis halts any g/p, hydrogel, formation like changing ferrous iron to ferric iron and losing the ability to carry oxygen in hemoglobin. Who knows? Regardless of your origin theory, you have a hard time denying the pathological findings of tissue damage. The rubber clots are found in about half of the deceased according to the Alabama embalmer Richard Hirshman. Tom Haviland sent out anonymous questionnaires to 179 embalmers world wide and about half would admit to seeing the rubber clots. So overall we need more people testing out potential treatments and sharing results.
Oh, clap your hands, all you peoples! Shout to God with the voice of triumph! Psm 47:1
Ronald, it’s comforting to know that there are other solutions. Dr. Ana Mihalcea seems to believe that only certain products work yet you’ve shown success with other products as well and this is encouraging for the public to know that there are more than one way to skin a cat so to speak.
Here’s an idea, although it might be harder to execute. Have you tried fasting? The body produces numerous enzymes when it’s in a fasting state, and this could very well have an equal, if not more potent affect on the g/p than any other solution. Have you considered fasting yet?
Also, i’m given to wonder if castor oil might also be another possible eliminator. If it has the ability to break down bone spurs, cysts , cataracts, and tumors with repeated applications via the use of castor oil packs, rubs, or drops then why couldn’t it also break down the spike protein and the g/p? Thoughts?
India ■ is said their country found urine to be the antidote for the virus; it is one's pee/morning best that their nation had a success of ridding this bioweapon. So I have heard. M