

Gel/plastic, Rubber Clot, Returns with this Change. Developing a Dose-Response Relationship
Gel/plastic, Rubber Clot, Returns with this Change. Developing a Dose-Response Relationship
Let me show the changes seen in my blood during various treatments.

Here is a 30 ml whole blood syringe test from 4 mths ago. This is a stock image of a syringe type test.

This is the actual gel/plastic (g/p), rubber clot from 4 mths ago. The volume of the g/p was 1.1 ml and rubber like.

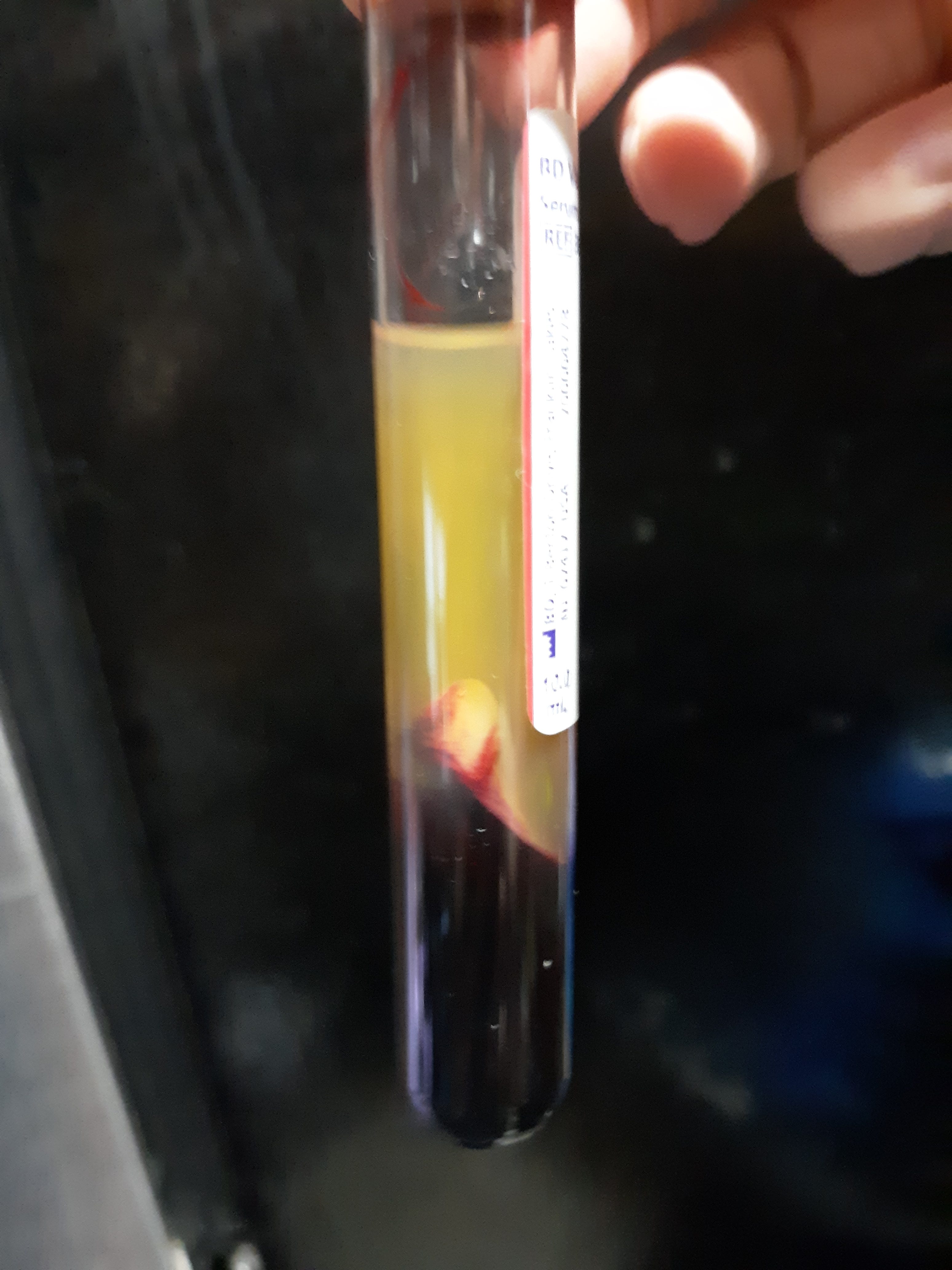
I started using 10 ml plain red top vacutainer tube and a centrifuge to demonstrate g/p, rubber clot. Here is a sample from 2 mths ago. The protocol for vacutainer testing is in the prior post.
The g/p collected this way when rinsed in tap water becomes whiter and rubber like in about 5 min after removal from the test tube. The following images demonstrate this.

To my surprise on 9/23 the red top plain vacutainer control tube with my blood did not show g/p, rubber clot to be present. It was by serendipity that I had added ivermectin and chlorine dioxide to my routine to try and lessen a sinus infection. I subsequently removed ivm for a week and added it back for a week and noted that when taking ivm for 5 days the g/p, rubber clot was absent and returned when I was off ivm. As I have previously stated, I cannot make any recommendations to anyone and check with your health provider when starting any treatment. The ivm dose I used was 1 ml (10 mg) daily taken orally of the type that is usually given as an injection of 1 ml for 110 lb body weight for cattle. My weight is 140 lb so this dosage is less than the 0.2 mg per kg used at beginning of the pandemic but was increased to 0.6 mg/ kg during delta variant by FLCCC type doctors.
As above I had also added chlorine dioxide (ClO2) at the time when I was trying to avoid a sinus infection. I do not recommend ClO2 to anyone. I hear that Mike Adams, The Health Ranger, uses it when he feels he is coming down with something and Dr Lee Merritt, The Medical Rebel, takes it daily but she also does not recommend it to anybody. In a recent test I continued the ivm and added a low dose of ClO2 daily to see what effect this had. This had the effect of clearing any cloudiness in the serum above the packed red cells in the tube. I did not know what the significance of the cloudiness was at the time but saw it when ivm was used alone without the ClO2.
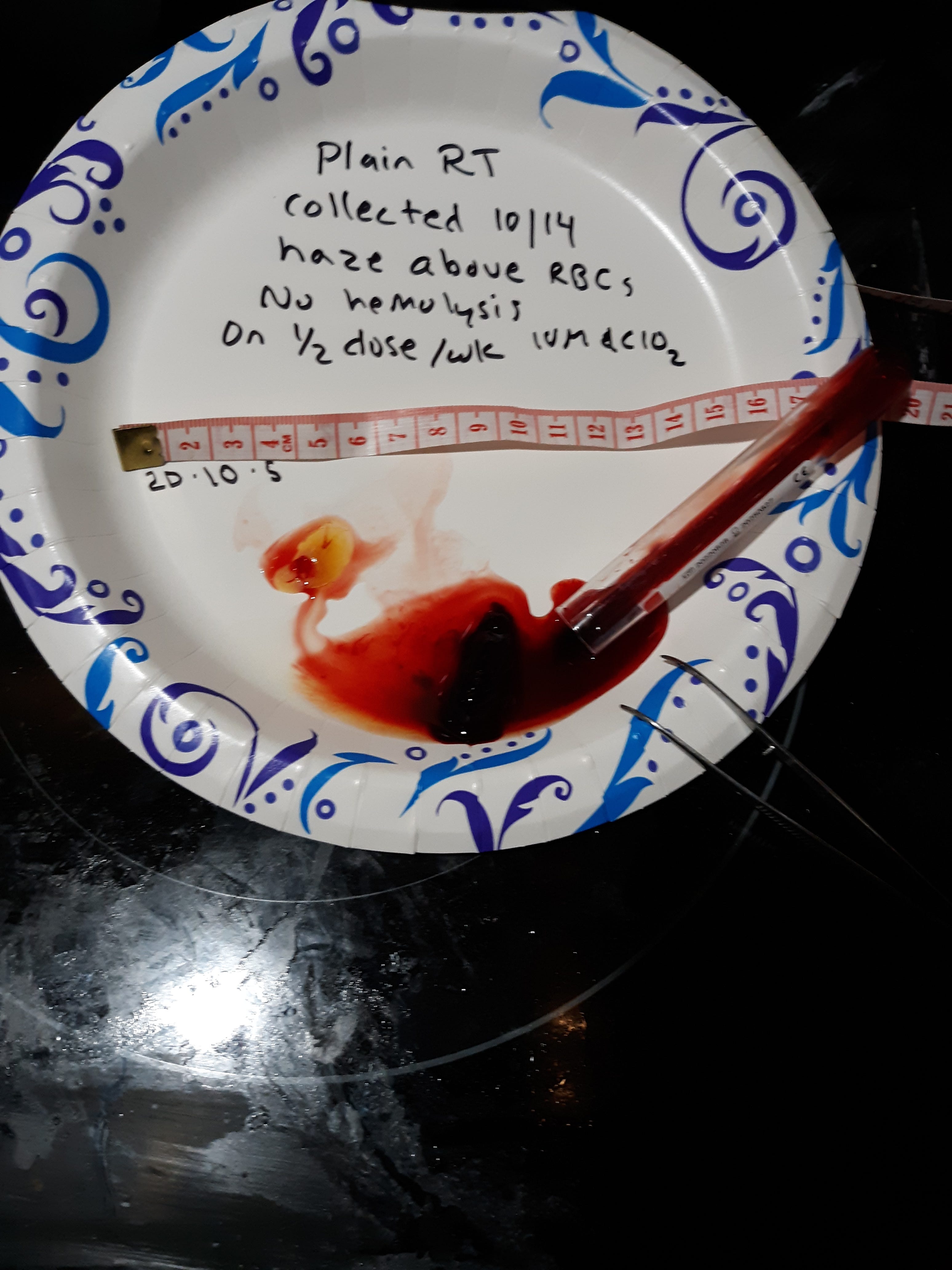
My most recent testing was to decrease the frequency of the ivm (10 mg) to every other day and to decrease the ClO2 (30 ppm × 4 ounces) frequency to every other day (taking one treatment not on the same day as the other). This decrease allowed the g/p, rubber clot, to return but establishing a dose/response relationship and further evidence as to a cause and effect for its use. The following picture shows this finding. Here is a picture of the plain red top tube with the cloudy appearing g/p above the packed cells following the centrifuge spin.

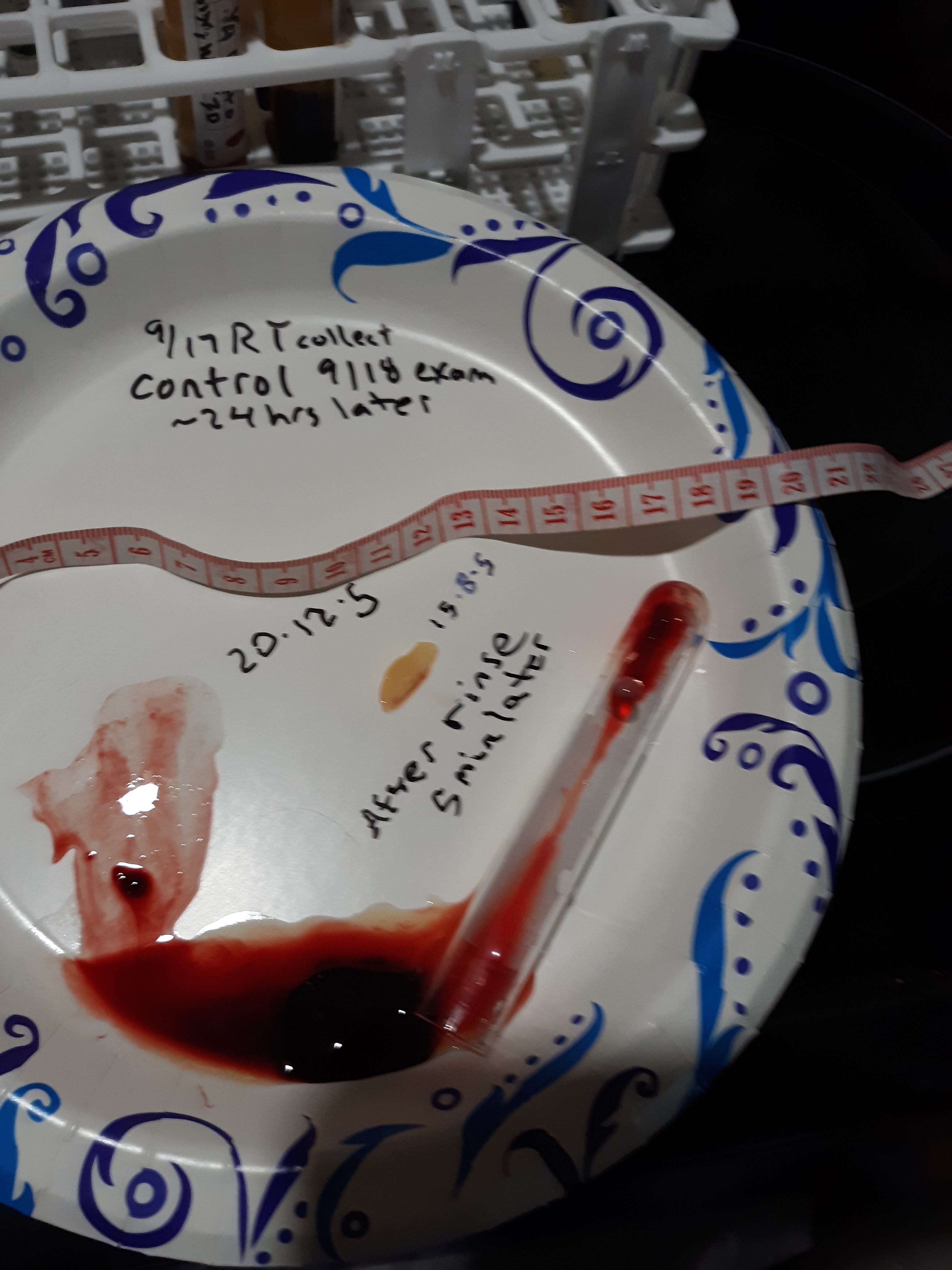
The following picture shows the contents of the tube with g/p, rubber clot.
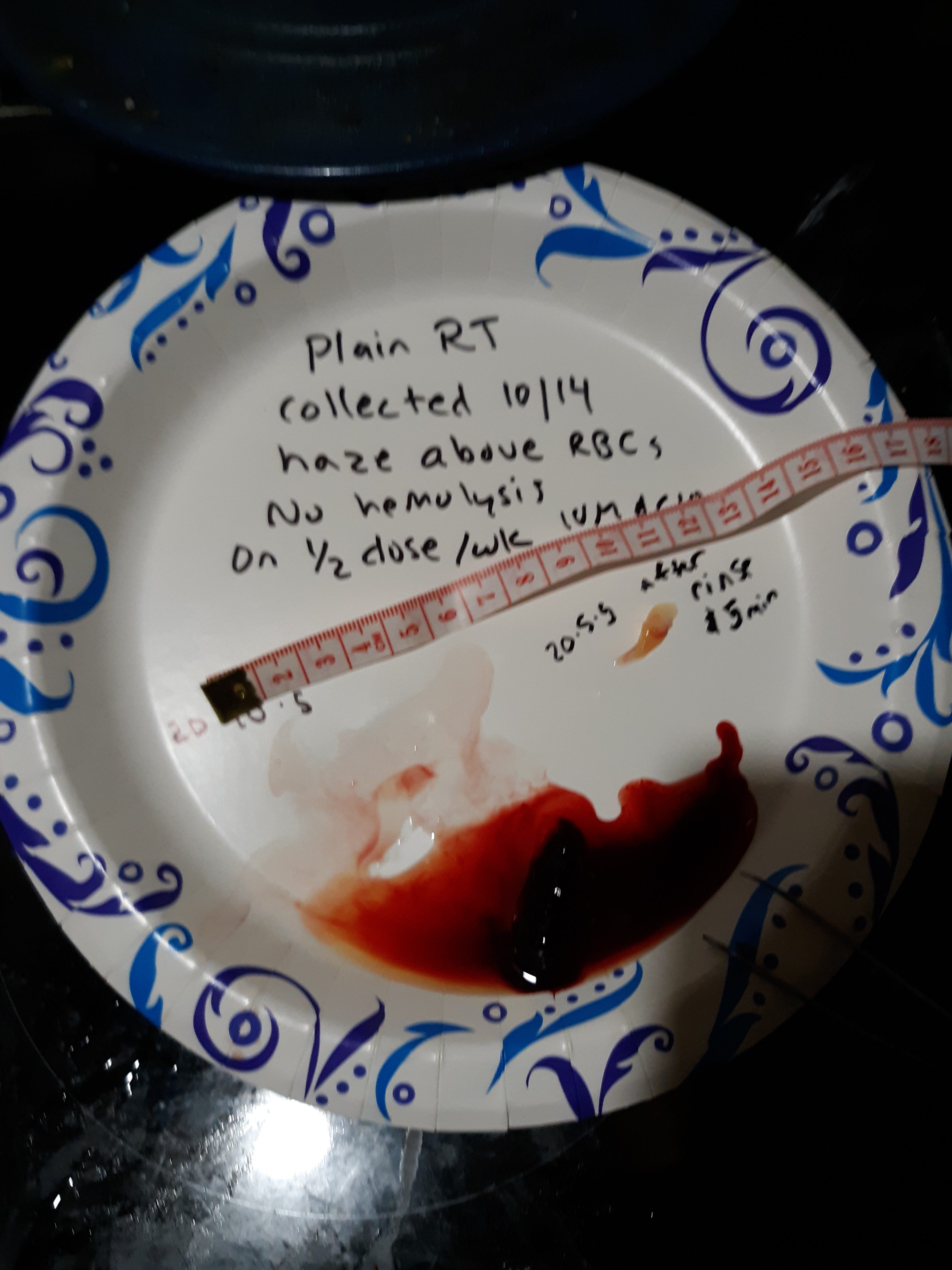
The following image shows the g/p, rubber clot, 5 min after removal from tube and rinsed in tap water. The volume has decreased and is now whiter and rubber like.
Here is a dark field at 40x showing 3-4+ rouleaux and a brownish fiber. This picture is what is present with my present findings of the return of g/p, rubber clot, following a reduced dosage of meds

.
Summary and discussion. Here is a list of what I was taking for months and was taking when I had g/p, rubber clot, by testing: vitamin d and c, iodine, proprietary zeolite, fulvic humid acid, methylene blue, melatonin, tumeric/ curcumin, NAC, dimethyl glycine, glutathione, quercetin, cod liver oil, and K2. I was also taking the 4 proteases (lumbrokinase, serrapeptase, nattokinase, and bromelain) as well as oral and topical EDTA. I can't say that these are not important and most have separate reasons to be taking them for good health. Interesting that I received a link from Dr Paul Alexander, (Hongjie, Front Cardiovasc Med 2022), that nattokinase of 10,800 FU/day x 12 mths managed progression of atherosclerosis and hyperlipidemia with no adverse side effects and the 3,600 FU dose was ineffective. In prior posts I showed each of the four proteases could digest fresh g/p, rubber clot, when placed in a saline solution containing any one of them and further prevented expression of g/p when added to my blood in a test tube. Again g/p is fresh if < 48 hrs from collection and it seems to be altered by time and/or formalin so is difficult to digest even with the above proteases over time.
EDTA binds metals and these are important components to many hydrogels and of course by definition the g/p is a hydrogel. Dr Ana Mihalcea is an advocate of EDTA. As above I am taking oral 400 mg EDTA daily and a topical EDTA daily with last intravenous EDTA two months ago.
IVM is important in the scheme of treatment since it inhibits spike at many levels. I don't know what spike is or how it gets into me but ivm blocks its targets at the ACE 2 and CD 147 level which inhibits many inflammatory processes like the cytokine storm and inhibits some blood clotting processes (The J of Antibiotics 75, 60- 71, 3022). Spike itself can form amyloid which appears to be a component of g/p when acted upon by neutrophil elastase to form amyloid fibrils (J Am Chem Soc 2022, 144, 20, 8945). For me it looks like I need to take 10 mg ivm at least daily since every other day did not prevent g/p from forming in my blood. By prior testing the 10 mg/ day did prevent g/p after I had been taking it for at least 5 days. I still think the proteases and EDTA are important (and maybe others) in prevention of g/p but further testing is needed.
For me personally I would take the proteases, EDTA, ivm, and maybe ClO2. I still am not sure of the need for ClO2 but will do testing with and without it. This is not an endorsement for you and so speak to your health care advisor prior to adding or changing your medications. Let me say that ClO2 at 30 ppm and a volume of 4 ounces is equivalent to 3.6 mg/ day. In the covid protocol by Andreas Kalcker he uses 30 mg / day, so is about 10 x more.
We need more people testing for g/p, rubber clot, and testing various therapeutics to try and narrow down what is effective.
Have mercy on us, O Lord, have mercy on us! For we are exceedingly filled with contempt. Psm 123:3
Hi Ronald,
Great work.
I do wonder what your next project will be after the G.P. is sorted? Perhaps we can even find out how to dissolve or excrete these fibres one day.
On Dr Annas last post it mentions the colonic irrigations expelling large amounts of gel and bundles of fibres. Coffee or edta enemas etc. Anything that removes large amounts sounds like progress.
Thanks and Regards, matt
Consider Bryan Ardis, DC's research of studies that show the SARS-CoV-2 spike protein is made from venom from two snakes. The two main actions of venoms are paralysis and blood clotting. Ivermectin bumps the spike protein (ie. snake venom) off alpha-7 nicotinic acetyl choline receptors on our cell walls... as does nicotine and acetylcholine (a neurotransmitter). Remedies that also clear this receptor site are licorice root extract and ashwaganda. Ardis's recent explanation is at https://thedrardisshow.com/the-antidote Dr. Mahalcea wants to see the live blood to prove these antidotes are effective, because one of her patients was using nicotine patches. IV EDTA cleared it up where nicotine did not. I still think it must be considered. I also think copper supplementation plays into the equation because it's instrumental in making acetylcholine, which imo, is the correct neurotransmitter to attach to our cells. These are all things to ponder. Wish I had a dark field microscope so I could contribute some evidence.