


A Harder Time to Achieve Remission, but New Insights Too
I thought I was making a few minor changes to the protocol to stop the expression of gel/plastic, rubber clot, but seemed impossible to return to the no rubber clot state.

The first change I tried was to stop the low dose chlorine dioxide for 5 days. I continued the ivermectin, MedFive EDTA product, and lumbrokinase ( also continued various “less important” nutraceuticals). I had stopped the Cl02 in the past and it did not affect a continued remission so I expected the same result but suprisingly found rubber clot to be present.
The test involves collecting my blood, known to contain rubber clot when not under treatment, in a 10 ml vacutainer test tube via venipuncture, gently invert tube x 10, remain upright for 30 min, centrifuge for 30 min, examine the tube contents by visualizing area above packed red cells for any cloudiness that would be suspicious for the hydrogel which is the gel/plastic, rubber clot. The tube is then placed upright in refrigerator overnight and examined in about 24 hours by dumping the tube contents out on a paper plate for exam. The following picture shows the findings.
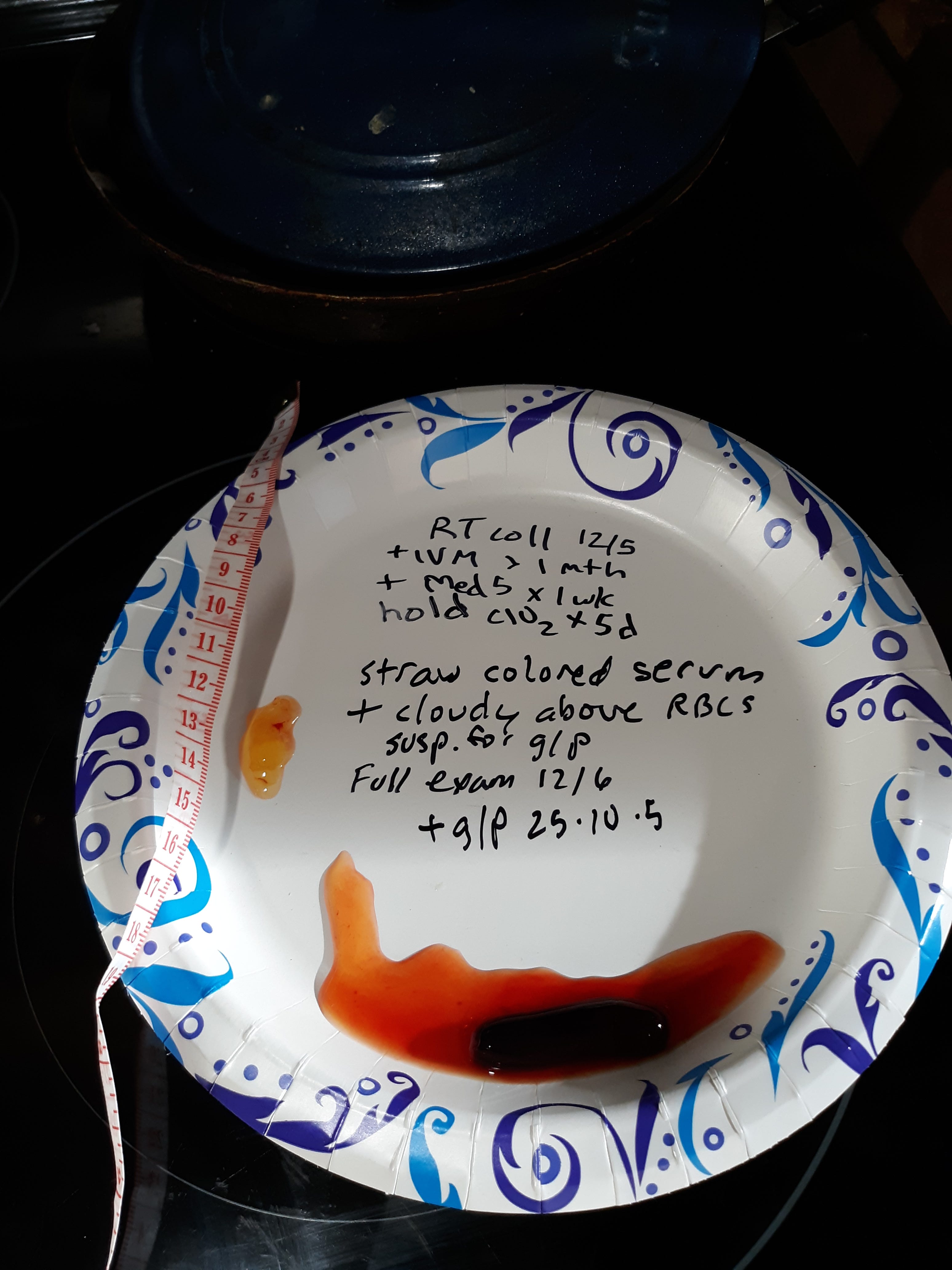
If the g/p is rinsed and allowed to dry for about five minutes it becomes more white and rubbery. Please see my prior posts for those images.
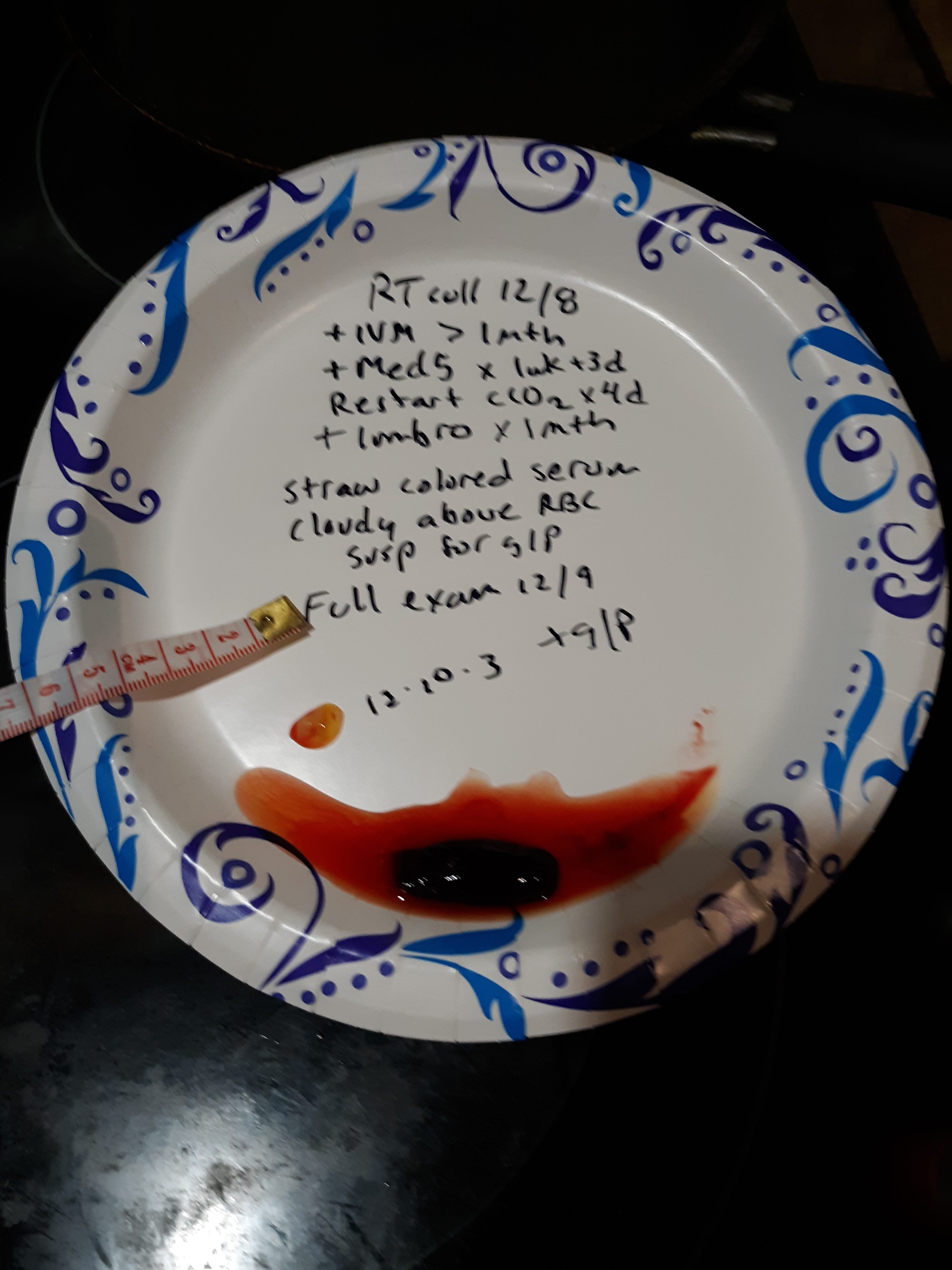
So it seemed logical to add back the Cl02 and repeat testing. The following picture shows results with the reintroduction of Cl02 for 4 days (30 ppm x 8 ounces/day). I had continued the ivm, MedFive product, and lumbrokinase plus less important nutraceuticals. The following picture shows the g/p, rubber clot, remains.
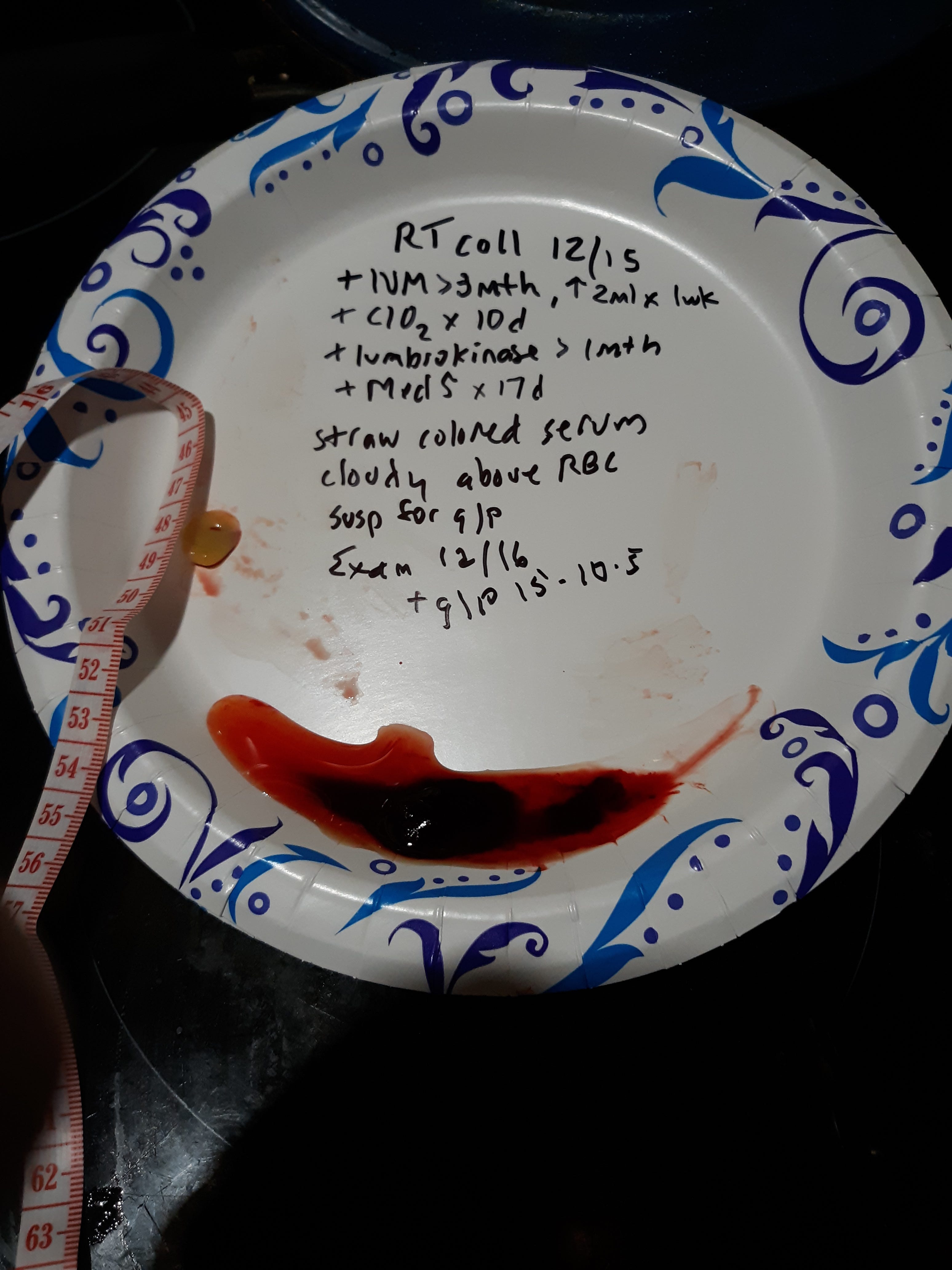
I thought that I should increase the ivm dose from 1 ml to 2 ml orally per day (20 mg). My weight is 140 lbs so this is about 0.3 mg/kg. Remember 0.2mg/kg was the initial dose of ivm but was increased to 0.6 mg/ kg for the delta strain. I continued the other compounds and still I had g/p, rubber clot present.
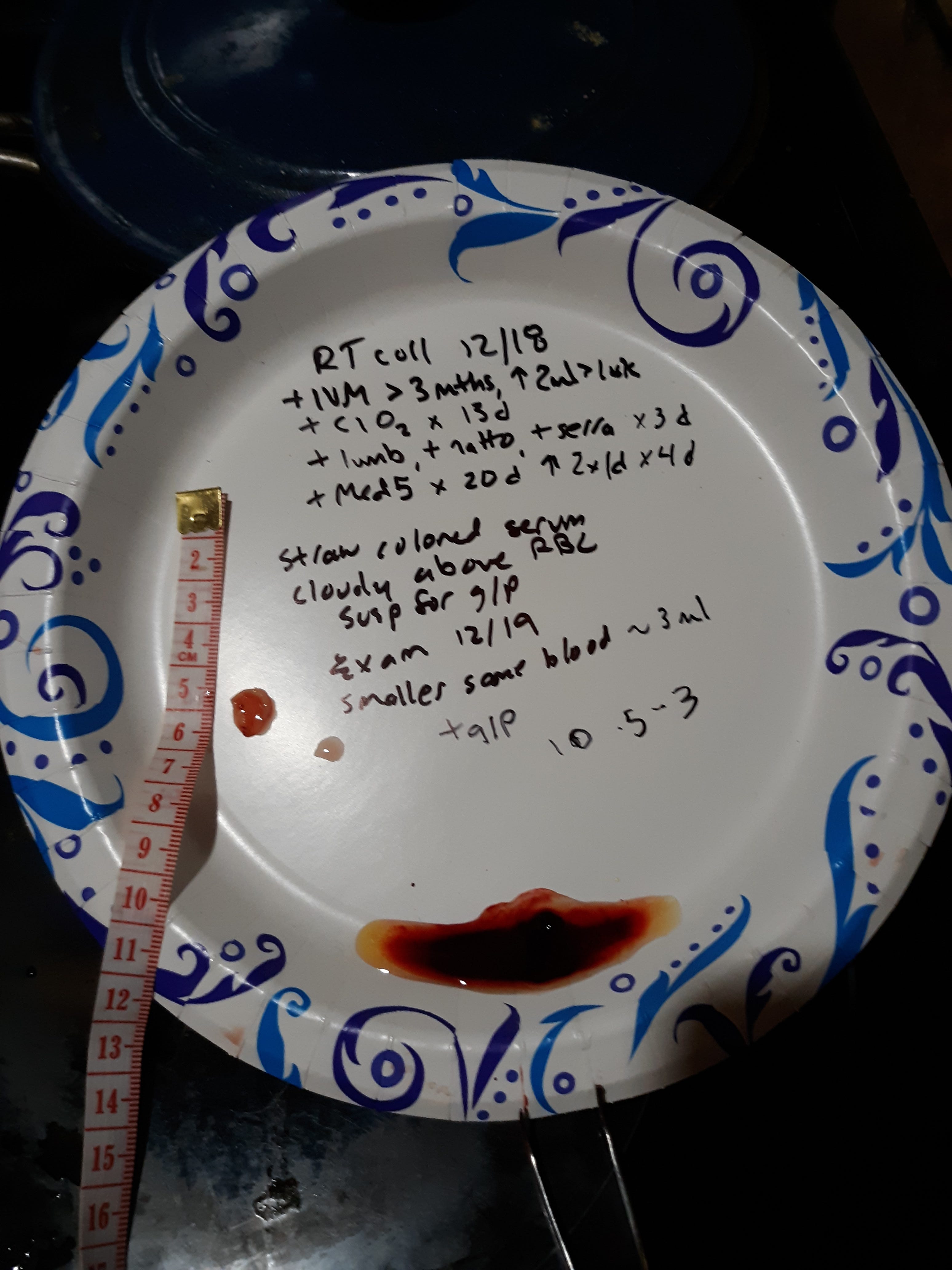
At this point I wondered how I could get back to remission, so I continued all the above plus added additional proteases such as nattokinase, serrapeptase, and increased the MedFive product to twice a day. The following picture shows the g/p, rubber clot, still present.
This did not make sense to me since this was even more products than what worked in the past. I wondered if the ivm was not effective since I had gone to a new container since it had ran out. I did notice that I was not having my personal side effect that I noticed when I was on 3 ml/ day and that is a slight seemingly brighter vision (lighter not sharper) and when I closed my eyes I would note a rising glow. This is hard to explain but when I searched for visual side effects of ivm I did not find any listed but that is what I had personally on a higher dose and was now absent with this container. I will say the prior ivm was a few months expired but I usually do not attribute potency to those dates. Maybe I'm wrong.
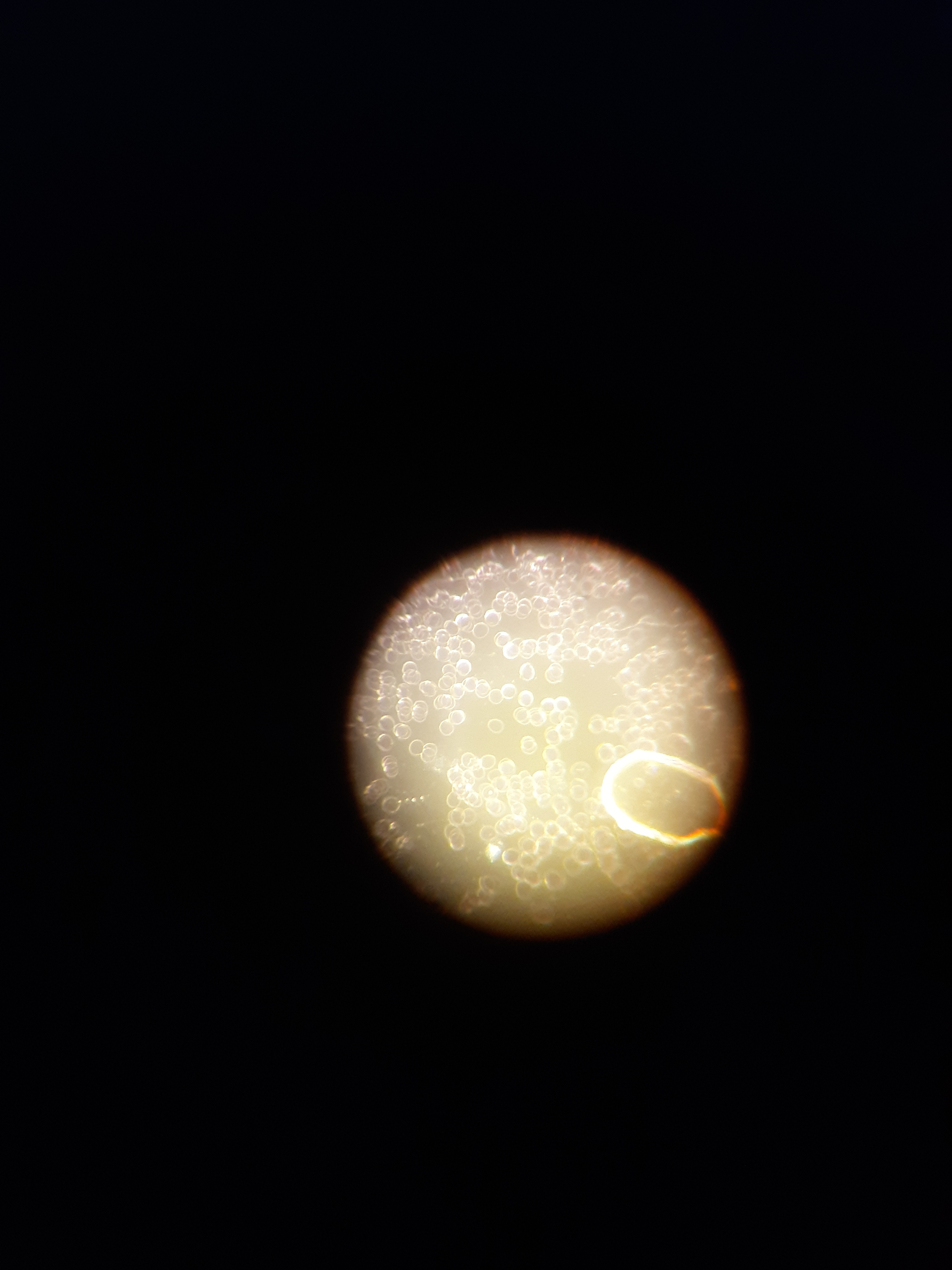
Well I took 3 ml of a new container and in a few hours had those visual effects that I tried to describe. I was feeling excited that I had found what the issue was, so I did a live blood analysis the next day to see what changes were now present. I had done several during this time and had noted 4+ rouleaux but now was at most 1+.
I waited an additional day and did a vacutainer test with use of the centrifuge to examine for g/p, rubber clot. The clear serum above the packed cells is noted in the following picture so no rubber clot present.
The following picture shows full examination of tube contents. No rubber clot present!
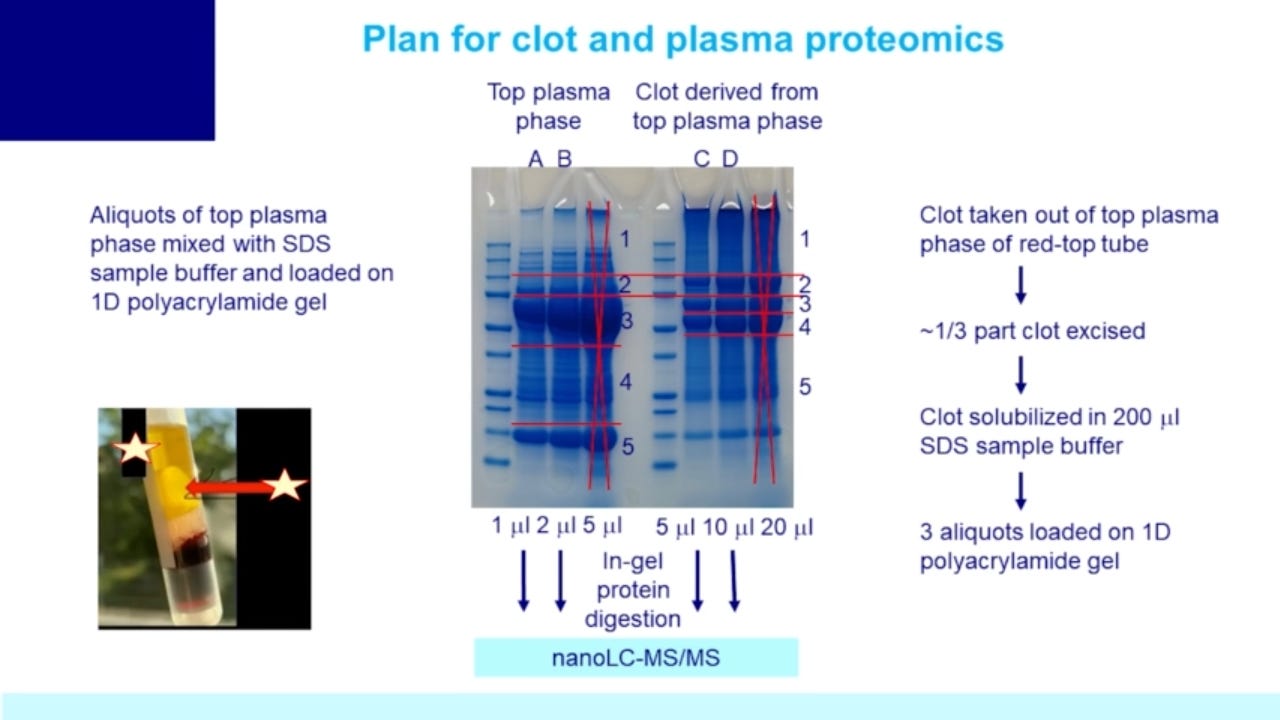
Summary and Discussion: l again refer to Dr Arne Burkhardt, the late German pathologist, that performed the first autopsy studies during this epidemic and found a endothelialitis (inflammation of inner wall of vessels). This inflammation resulted from spike protein (or whatever your flavor of nanoparticle) being produced in cells of the vessels and being attacked by your lymphocytes (an autoimmune disease). The damaged tissues released a protein mix of spike, amyloid fibrils, and structural protein fragments. Here is the link to Dr Burkhardt on rumble: https://rumble.com/v2h5zuy-pathologist-dr.-arne-burkhardt-autopsies-show-the-mrna-vaccine-shreds-peopl.html
In Dec of 2021 Dr Burkhardt presented his findings of an autoimmune destruction from autopsy studies to a symposium for the Doctors of Covid Ethics in the UK. In January of this year he made reference to several papers connecting spike to an amyloid/hydrogel mix.
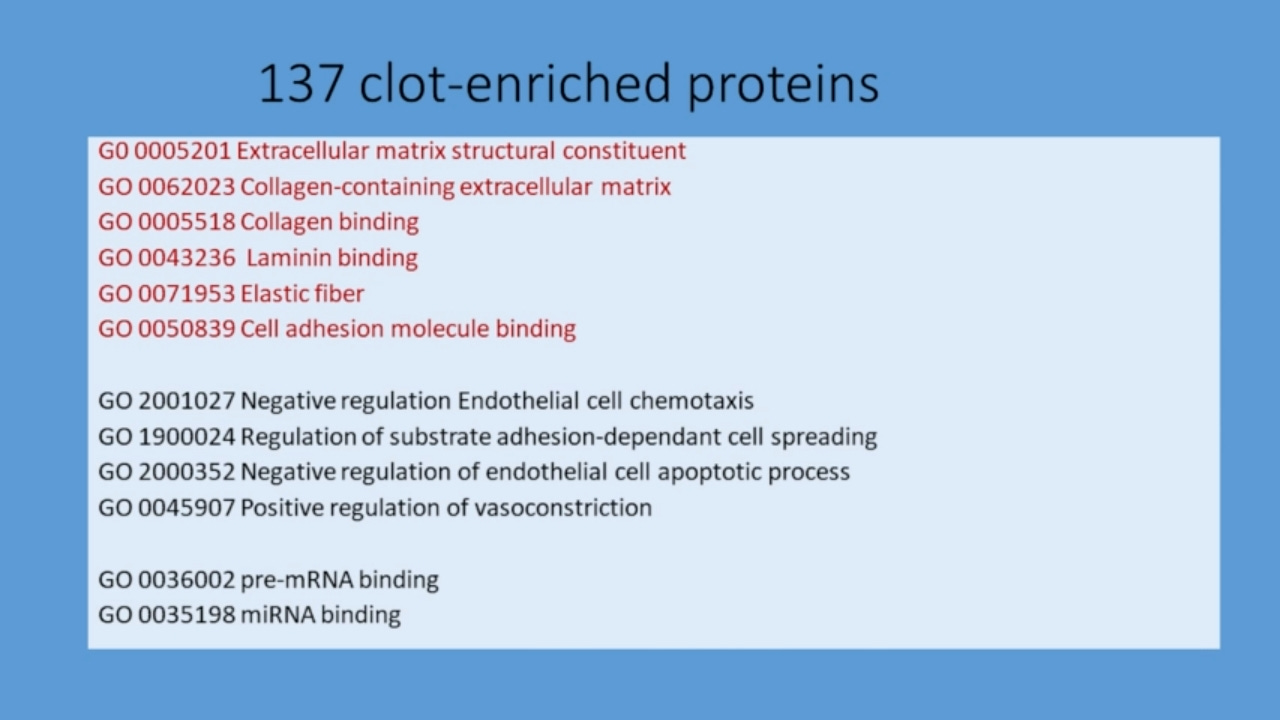
J Am Chem Soc 2022, 144, 20 reports the theoretical prediction of 7 amiloidogenic peptides in spike. The following two pictures are from Dr Burkhardt's presentation.
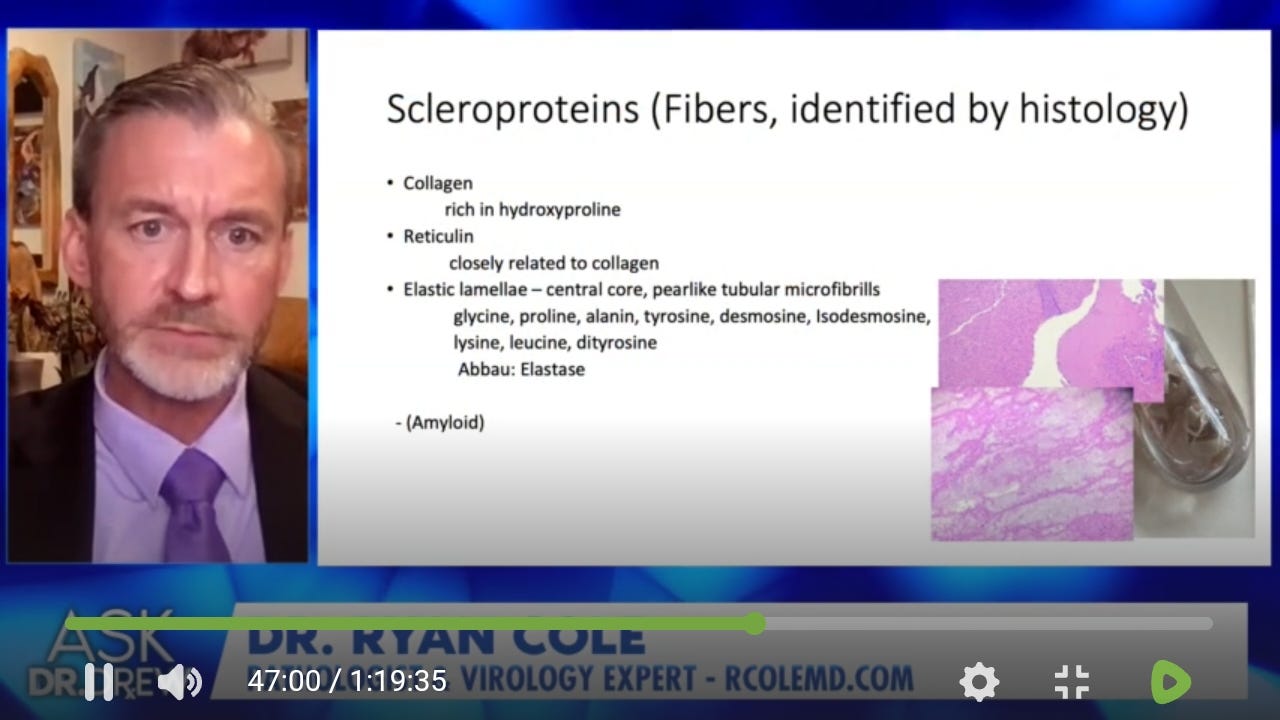
Additionally Dr Ryan Cole in the following slide shows the components of the rubber clot he calls scleroproteins.
As I stated in prior posts I am here to share my findings freely and no product to sell, but the personal treatment is not a recommendation to you. Please do your own research and by all means testing to confirm or refute any claims. I know from these recent results that I need to do frequent live blood analysis to follow treatments and to confirm with in vivo testing using vacutainer tubes and a centrifuge. I think the overall treatment is similar to Dr Peter Mccullough and Dr Pierre Kory with nattokinase, bromelain ( proteases), curcumin, and NAC (augmented is best) with ivermectin and MedFive product added. The MedFive product contains EDTA and Dr Ana Mihalcea is an advocate of EDTA. Now, I still need to narrow down the essential products required to sustain remission from the rubber clot formation. It seems to me the best treatments will be directed against the inflammatory process that results in the amyloid /hydrogel product of tissue destruction. If the inflammation is not addressed as seen in the pathological findings then treatment of the amyloid/hydrogel precursors to rubber clot formed after tissue destruction may not improve prognosis and conditions like SADS (Sudden Adult Death Syndrome) may not decrease. I have made reference to how ivm stops inflammation associated with spike. Some of the mechanisms of ivm can be found at J of Antibiotics, The Mechanisms of Action of Ivermectin Against SARS CoV 2, 75, 60 -71, 3022. Remember it can inhibit binding of spike to ACE 2 receptor on the endothelium and inhibit multiple pathways leading to a cytokine storm (inhibition of MAP 3 kinases, NF kb, STAT 3, PAK 1 and more!) It also blocks spike binding to CD147 receptors on red blood cells and likely reducing rouleaux formation as was seen in this testing. Ivermectin remains on the WHO list of essential meds and received a Nobel prize for its discovery in 2015. Its intermittent use is well established but less known about any prolonged daily use. It has a long half life and is lipid soluble so accumulation in some tissues is probable. It concerns me that some batches may be less effective / potent. I know you may have additional questions on hydrogel and in my prior post I addressed this aspect. We need more of us testing ourselves with different treatments to find solutions!
Merry Christmas and Peace on Earth with Goodwill to Men. Amen
I believe that prayer draws on energy that exists and energy that is created. In utilizing energy that exists, by simply asking, we can boost our arsenal.
In creating new energy we can initiate. Start demanding that the clots dissipate. Mentally call on the strongest thing that you know to destroy and conquer. Envision your body defeating the spike. Ask God, who ever you believe Him/Her to be, to give you the energy to heal. Just ask. What could it hurt? You are open minded enough to observe any differences.
Happy Christmas! And a blessed and healthy New Year!
The spike is just..evil..all the ways it can mess people up.
May your protocol continue to work for you. Thanks much for sharing your results.